
Should we call the condition of elevated glucose toxicity “prediabetes?”

No
This just might be the worst use of branding in medicine to-date. The prediabetes label is quite likely creating significantly more problems than it is solving. By calling the initial stages of elevated glucose toxicity “prediabetes,” the medical community is attempting to scare people into behaviors that stop them from advancing to having extreme levels of glucose toxicity (i.e., full-on diabetes). But, I fear, the exact opposite is happening (bear in mind, this is anecdotal, as I have myself, my friends and my colleagues who are prediabetic from which to base this on).
The diagnosis of prediabetes telegraphs that you are still basically OK (i.e., you are in a prior-to-diagnosable condition), but that you need to do a better job managing your glucose so that you do not progress to the “magic threshold” of a 6.5% A1c, at which point you are diagnosed diabetic.
For one, suggesting that you are generally healthy as long as you’re below an A1c of 6.5 is a problem (because you’re not). Also, embedded in this message is that you’re not in a diabetic state, and therefore, still technically healthy. Just adjust your lifestyle a bit and you’ll probably be OK.
The problem is that this warning backfires too easily. Here’s the actual impact on a patient of this poorly-branded diagnosis: “Whew! I’m not diabetic. That’s good. And to avoid diabetes, I’ll do my best to skip that soda and that pasta… when I can. That should do the trick!”
Sadly, this does not do the trick. Any possible adherence to a more strict diet doesn’t stick, because there is no awareness of the damage being done even in the so-called prediabetic state. And, frankly, with no obvious pain or discomfort as a result of glucose toxicity at moderate levels, there’s nothing holding a prediabetic person any more accountable to effective glucose management techniques as what holds the average person to any diet over the long-term. People generally stink at sticking to diets.
Boiling it down, the therapy for being diagnosed as prediabetic is diet and exercise. What a fool’s errand to rely on such an unreliable and difficult-to-sustain tactic to address something so potentially harmful. What is actually happening is that prediabetics are lulled into a feeling of “I’m actually OK for now” yet are, in fact, inflicting damage on their internals over the long-term (especially for those “pre-diabetics” who have A1c’s over 6!) because the message is “You’re OK right now. Watch what you eat.” when the message ought to be “Your glucose levels are elevated, which means that even in small ways, you’re doing long-term damage to your internals. If you don’t keep tabs on your glucose levels on a regular basis, you will most likely suffer from permanent, painful complications if you’re lucky enough to live to a ripe old age.”
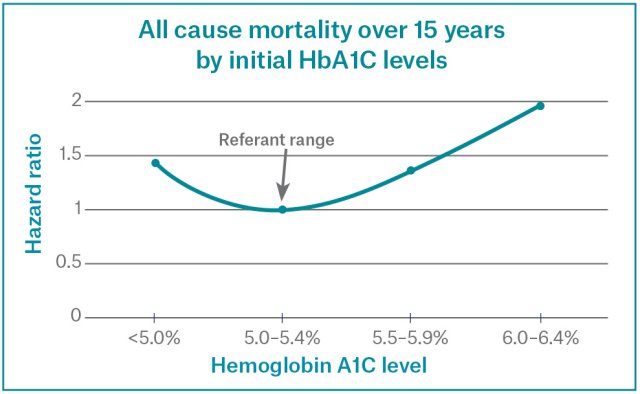
The reality is that any A1c over 5.5 is inviting increasing risk of complications due to glucose toxicity. To be fair, the significantly elevated risks that lead to permanent damage start occurring at 6.0 A1c, but there are studies that show increase in probability in health problems starting at 5.5 A1c (don’t get me started on endocrinologists who have some secret handshake to all agree that anything “under 7 A1c is good control for a diabetic” – infuriating, patronizing, and wrong. OK, you got me started – more on this below in The Healthcare Industry Predicament later in this document).
{kind=link}
Yet, prediabetes is currently defined in the medical community as an A1c of 5.7 – 6.4. This means that through this entire range, people are already doing some potential damage to their system that cannot be undone. Worse, those on the higher end of prediabetes are doing far more potential damage to their systems that most likely will impact their livelihood if they are lucky enough to live a long life.
Recommendation:
The medical community should stop using the term prediabetes, which is just another unhelpful coined name that allows us to not think about what it means or worry about what’s behind the label.
What should we call prediabetes, then? The recommendation is to call it what it is: an insulin resistance disorder. However, because this is the low-end/entrypoint of the disorder, we can leverage a term from other medical diagnoses – a term that people already understand because it is clear and descriptive – to help clarify the type of insulin resistance disorder this is:
Pre-diabetes is a stage one
insulin resistance disorder.
Makes sense, right? It’s clear, descriptive, and harmonizes with how we use “stages” in other diagnoses.